Snoring Treatments
Snoring and OSA
Almost 50% of people snore at some point in their lives.
Snoring is more common in men, though many women snore. It appears to run in families and becomes more common as you get older. About 40 percent of adult men and 25 percent of adult women are habitual snorers. Men become less likely to snore after the age of 70.
So, what is snoring? To put it simply, snoring is the unpleasant sound that can occur as you sleep. Snoring occurs when you breath in and the flow of air causes tissues in the back of your throat vibrate. The sound can come through the nose, mouth or a combination of the two. It can occur during any stage of sleep.
Sleeping on your back may make you more likely to snore. It may also occur as your throat muscles relax from use of alcohol or other sedatives or relaxants. Nasal obstruction caused by viruses, allergies or sinus disease can also cause you to snore.
Snoring can be a nuisance to anyone who sleeps near you. You may even snore loudly enough to wake yourself up. Though, in many cases people do not realize that they snore. Snoring can also lead you to have a dry mouth or irritated throat when you wake up.
Health Risks
Light snoring may not disrupt your overall sleep quality. Heavy snoring may be associated with:
- Obstructive sleep apnoea (OSA)
- A serious sleep disorder and a risk factor for heart disease
- Stroke
- Diabetes
- and many other health problems.
OSA is diagnosed by appropriate sleep studies detecting long pauses in breathing (apnoea) or episodes of limited airflow (hypopnoea). Oxygen levels in the blood drop during these events which causes many problems around the body.
Coverage
If you are considering a consultation with us regarding snoring, it is worthwhile having a pre-consultation sleep study to determine the severity of the disease we are treating. Severe disease may qualify for DHB funded treatment options. Some insurance companies are no longer funding some surgeries for treatment of OSA. Treatment of just simple snoring without sleep apnoea is usually not funded by insurance; however, surgery for nasal obstruction not responding to medical treatments is covered by most insurance companies.
Treatment
I no longer offer office-based treatments despite my initial enthusiasm.
Office-based treatment of snoring is considered the “Holy Grail” of snoring treatments. Since 2001 when I started private practice, I have tried many office-based techniques to help stop simple snoring.
These treatments include:
- Injection snoreplasty
- Radio frequency treatment to the soft palate
- Pillar implants
- And others.
All are aimed to create some scarring of the soft palate to stiffen it—therefore, less snoring. However, although this seems to be an attractive idea, when I audited my results in the longer term over 15 years, the success rate is roughly 50%. Like tossing a coin! Although we got a lot of successes, there were some who had minimal response, or relapsed later and occasionally very few were worse.
For people with simple snoring without significant OSA, I am offering day surgery coblation assisted uvuloPalatoplasty (CAUP), although the costs are higher than office-based techniques and require a general anaesthetic, as the success rate is more predictable.
Uvulopalatopharyngoplasty (U3P) & Tonsillectomy
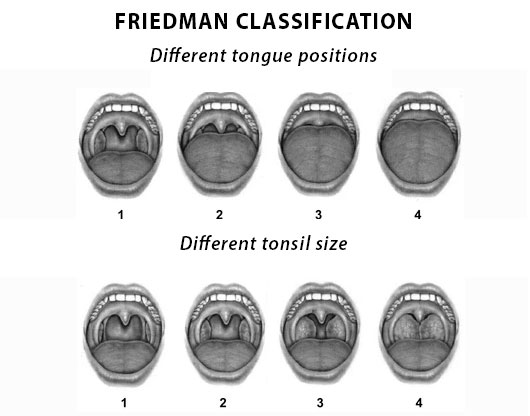
Surgery to the soft palate such as modified uvulopalatopharyngoplasty (U3P) and tonsillectomy have very high success rates for control of snoring with OSA, often quoted as greater than 80% for the right patient. However, to be that right patient, you need to have large tonsils and a small tongue (Friedman Classification 1,2). “Classical” U3P in unselected patients has a poor success rate.
That’s why it is crucial that a good clinical assessment of your anatomy is done before we discuss suitability for surgery. The key things are tonsil size, tongue position and body mass index (weight). Nasal breathing is important. The inability to breathe easily through your nose at nights makes you often sleep with your mouth open and this then leads to instability of the relaxed tongue and reduction of the airway space with palatal and tongue base vibrations.
People with larger tongues (Friedman Classification 3,4) often need reduction in the volume of the tongue in association with Modified U3P to obtain a reasonable chance of surgical success. Occasionally, other treatments are required such as removal of lingual tonsils, palatal advancement, maxillo-facial surgery.
Continuous Positive Airway Pressure Treatment (CPAP)
CPAP, or continuous positive airway pressure treatment, is another good, well recognised treatment for OSA. This is a mechanical device to supply airflow into the nose or mouth at night to support the collapsing airway. However, this is not a treatment for everyone, and ability to tolerate the device varies in the literature from 30-60%.
I was recently disappointed to see a university student in my rooms who had been diagnosed with OSA by a “sleep clinic” and told to buy a CPAP machine for several thousand dollars. He had large tonsils and adenoids which had been overlooked, and a single surgery cured him, with normalization of his sleep study. He didn’t enjoy using the machine and now, especially after a surgical cure, his purchased machine was redundant. Clearly a team approach to OSA is a real benefit to patients, and we have a good working relationship with respiratory physicians in Christchurch who are extremely helpful in the treatment of OSA.
Oral appliances or mandibular advancement splints (MAS) are useful in the treatment of simple snoring and some cases of OSA. They work by moving the lower jaw forward at night thereby moving the tongue forward and increasing the posterior airway space. The cost of these devices varies from $100 like the internet special boil and bite mouthguards, to $370 for the Apnoea RX from Harvey Norman, to approximately $1000- $2000 to the low profile dentally fitted appliances which have less long-term effects on your bite and better tolerance.
During your consultation and assessment, we will be discussing all these options and try to work out which treatment will be the best fit for you.